Early Repair of Shoulder AC Joint Key to Recovery
You have a bump on your shoulder after a fall. You are told you have a shoulder separation or AC joint dislocation. Now what do you do?

Understanding AC Joint Bumps and Their Causes
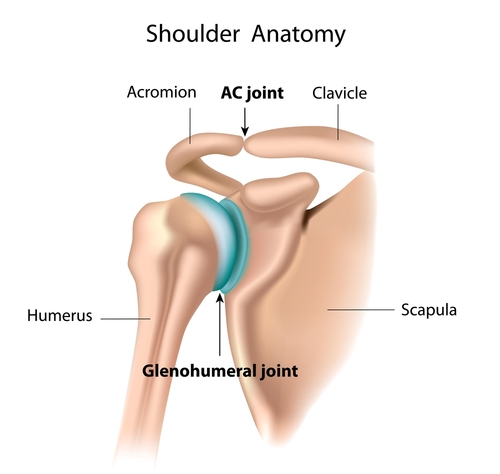
A shoulder separation is an injury to the acromioclavicular (AC) joint on the top of the shoulder, where the collarbone (clavicle) meets the highest point of the shoulder blade (acromion). An injury to the AC joint is common, often caused by a blow to the shoulder or a fall onto an outstretched hand. The fall injures the ligaments that surround and stabilize the AC joint, forcing the clavicle to detach from the acromion. This creates a bump or bulge above the shoulder. The shoulder and neck muscles contract a bit as the shoulder no longer has the strut of the clavicle to hold it out to length and provide normal stability. Many of the NFL linemen have an AC Joint injury and chronic separation.
Effective Treatments for AC Joint Bump
The AC joint separations are divided into various categories depending on the severity of the damage. Mild AC joint injuries (Type I and II) may respond to conservative treatment such as ice, a sling, and physical therapy. More severe injuries (Type III, IV, V, and VI) are usually treated with surgical repair. When these ligaments are badly torn, they never heal on their own because the clavicle is elevated past the healing distance of the torn ligaments. Why fix them? Because the clavicle’s connection to the acromion provides a stable strut against which the entire shoulder can be leveraged. When damaged and dislocated, many people will notice the loss of strength and mild pain in the shoulder as it is not as stable as before the injury. The long-term outcome of a dislocated AC joint is painful arthritis at the AC joint itself, which is somewhat puzzling since the clavicle is displaced outside the joint. However, it appears that abnormal forces and motions, which intermittently cause the clavicle to interact with the acromion, lead to the degenerative change over time. The early restoration of the AC joint may prevent this subsequent AC joint arthritis.
Will an AC Joint Bump Go Away on Its Own?
There remains some controversy about the best way to treat Type III shoulder separations. Although some patients and doctors choose the non-operative option, athletes who are overhead throwers or who play tennis, volleyball, and squash, are significantly weakened by a Type III joint dislocation for up to a year after injury and are often mildly affected permanently. Knowing this, many of our athlete patients choose to have the injury repaired. The rationale for early repair is that freshly torn ligaments can be sutured back together and backed up by wrapping an allograft or donor tissue around, and sometimes through, the elevated clavicle.
The repairs work well however there is still a failure rate due to tissue stretching or bone weakening. Multiple types of repairs have been designed including plates with screws into the bones, bands of artificial material connected to metal dog bone-shaped retention devices, and other artificial material combinations. Unfortunately, many of these pull through the bones. We prefer to use donor tissue to reproduce, as closely as possible, the normal anatomy of the damaged ligaments, backed up by suture band material and augmented with growth factor injections after surgery. AC Joint repairs are outpatient procedures performed under a local regional block. The procedure uses natural tissues, which provide excellent stability for the AC joint. It is, in our opinion, the safest and strongest way to rebuild the AC joint with the lowest complication rate. Possible complications can be loss of fixation or loss of stability, which most commonly occurs when a patient has a repeat fall during the early healing period.
Comprehensive Approaches to AC Joint Separation Recovery
A great rehabilitation program beginning immediately after surgery is crucial to a full recovery. On day one after surgery, a soft-tissue massage to the neck and surrounding musculature is initiated immediately as well as a total body-conditioning program designed to return the athlete fitter, faster, and stronger than they were prior to the injury. Stationary bike, core exercises, and scapular stabilization exercises are used to initiate a cardiovascular workout on day one with the goal of keeping the patient feeling like an athlete in training rather than a patient in rehabilitation. A prompt repair and focused rehab can ensure a rapid return to full activities usually by three months after repair. Significant AC joint injuries are another example of how conservative care should mean early repair, not non-operative care, when the critical torn tissues can be fixed.
Article originally published June 4, 2014. Updated & republished September 6, 2020 by Kevin R. Stone, MD with scientific and content updates.
Here's Dr. Stone's Advice on the Best Approach to AC Joint Repair
If you would like to find out more about a shoulder injury you're experiencing, use our Shoulder Pain Symptom Checker